In This Guide
Let's be honest, talking about period pain can feel awkward. But when the pain is so bad it makes you miss work, cancel plans, or just curl up in bed for days, it's time to stop calling it "just cramps." For millions of women and people assigned female at birth, that debilitating pain has a name: endometriosis.
I remember a friend describing her journey. She spent years being told her agony was normal, that she had a low pain tolerance, that she should just take an extra ibuprofen. It took a decade and seeing seven different doctors before someone finally listened and she got a diagnosis. That story? It's frustratingly common. And it's why understanding endometriosis matters.
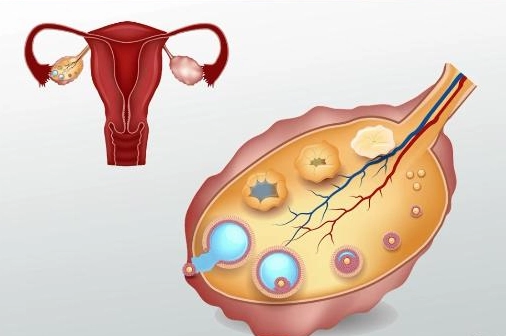
So what is it, really? In simple terms, endometriosis is a condition where tissue similar to the lining of the uterus (the endometrium) decides to grow in places it absolutely shouldn't. Think your ovaries, fallopian tubes, the outside of your uterus, your bladder, or even your intestines. This tissue isn't just misplaced; it's rebellious. It acts like regular uterine lining—it thickens, breaks down, and bleeds with your menstrual cycle. But with no way to exit the body, it gets trapped. Hello, inflammation, scarring (adhesions), and pain that can range from "uncomfortable" to "I can't move."
Why This Guide is Different
You'll find plenty of medical websites with dry lists of symptoms. This isn't that. We're diving into the messy, confusing, and very real experience of living with or suspecting you have endometriosis. We'll talk about the symptoms doctors miss, the emotional toll of the diagnostic odyssey, and the practical pros and cons of every treatment option—not just the textbook version.
Beyond the Cramps: The Full Spectrum of Endometriosis Symptoms
If you think endometriosis only causes period pain, you're missing most of the picture. The symptoms can be all over the map, which is a big reason diagnosis is so tricky. The classic sign is pelvic pain, often worse during your period (dysmenorrhea). But let's break down what that pain can actually feel like, because "pain" is a pretty useless word on its own.
For some, it's a deep, aching throb that settles in the lower back and pelvis. For others, it's sharp, stabbing pains that take their breath away. The pain might radiate down the legs. It often gets worse around ovulation and, of course, menstruation. But here's the kicker—for many with endometriosis, the pain doesn't stick to a calendar.
What Does Endometriosis Pain Feel Like? People Describe It As...
- A hot knife being twisted in your pelvis.
- Constant, deep bruising that never fades.
- Glass shards scraping inside you with every movement.
- Your organs are glued together and being pulled apart.
It's more than just a "bad period." It's a systemic issue.
Then there's the pain with intercourse (dyspareunia). This is often deep pain, not superficial, and it can be severe enough to make sexual relationships incredibly stressful. Bowel and urinary symptoms are huge red flags that often get misdirected to gastroenterologists or urologists first. We're talking about:
- Painful bowel movements, especially during your period.
- Diarrhea, constipation, or cycling between both around your cycle.
- Bloating so severe it's nicknamed "endo belly"—where your abdomen distends painfully, sometimes for days.
- Pain when your bladder is full or a frequent, urgent need to urinate.
Fatigue is another massive one. It's not just "I'm tired." It's bone-deep, crushing exhaustion that sleep doesn't fix, often made worse by chronic pain and inflammation.
And we can't skip infertility. While not every person with endometriosis struggles to conceive, it is a common challenge. The inflammation and scar tissue can interfere with the function of the ovaries, fallopian tubes, and uterus. It's a heartbreaking layer on top of everything else.
What's wild is that the severity of symptoms doesn't always match the amount of visible disease. Someone with minimal, superficial lesions (Stage I) might be in excruciating pain, while someone with extensive scarring and ovarian cysts called endometriomas (Stage IV) might have milder symptoms. This disconnect baffles doctors and invalidates patients all the time.
The Long, Frustrating Road to an Endometriosis Diagnosis
This is where the system often fails people. The average delay in diagnosis is still between 7 to 10 years. Let that sink in. A decade of pain, confusion, and being told it's in your head. Why does it take so long?
First, the symptoms overlap with a dozen other conditions (IBS, pelvic inflammatory disease, interstitial cystitis). Second, many primary care doctors and even some gynecologists aren't adequately trained to suspect it. Third, and this is a big one, there's no simple, non-invasive test. You can't diagnose it with a blood test or a standard ultrasound with 100% certainty.
So what does the diagnostic process look like? It usually starts with a very detailed conversation about your symptoms and their pattern. A pelvic exam might reveal tenderness or nodules behind the uterus. Imaging like a transvaginal ultrasound is helpful—it can spot tell-tale signs like endometriomas ("chocolate cysts") on the ovaries or deep nodules. But a normal ultrasound doesn't rule out endometriosis. It can miss superficial disease.
A Major Myth to Debunk
Myth: "If your ultrasound is clear, you don't have endometriosis."
Truth: This is flat-out wrong and leads to countless missed diagnoses. Superficial peritoneal endometriosis, a very common type, is often invisible on ultrasound. The only definitive way to diagnose it is through laparoscopic surgery with biopsy.
That brings us to the gold standard: diagnostic laparoscopy. It's a minimally invasive surgery where a surgeon inserts a tiny camera through a small incision in your belly button to look directly at your pelvic organs. If they see suspicious tissue, they can take a sample (biopsy) to confirm it's endometrial-like tissue. This surgery is both a diagnostic and often a therapeutic tool, as surgeons can excise (cut out) or ablate (burn) the lesions they find.
Finding a doctor who specializes in endometriosis is crucial here. A general OB/GYN might not have the advanced surgical skills to properly recognize and remove all types of lesions, especially deep infiltrating endometriosis (DIE).
Your Treatment Toolkit: Navigating the Options for Endometriosis
There is no cure for endometriosis. I wish I could say differently, but it's true. The goal of treatment is to manage pain, slow the progression of the disease, improve quality of life, and preserve or enhance fertility if that's a goal. Treatment is highly individualized. What works wonders for one person might do nothing for another. It's often a process of trial and error, which is frustrating but real.
Let's lay out the options, from least to most invasive.
1. Pain Management and Anti-Inflammatories
This is usually step one. Over-the-counter NSAIDs like ibuprofen or naproxen can help reduce inflammation and pain. The key is to take them before the pain becomes severe—following a schedule around your cycle, not just when you can't stand it anymore. For some, this is enough to manage. For many, it barely scratches the surface.
2. Hormonal Therapies: The Mainstay of Medical Management
Since endometriosis tissue responds to estrogen, many treatments aim to lower estrogen levels or stop ovulation to suppress the lesions. Think of it as putting the disease to sleep.
| Treatment Type | How It Works | Pros & The Good Stuff | Cons & The Not-So-Good Stuff |
|---|---|---|---|
| Combined Hormonal Birth Control (Pill, Patch, Ring) | Prevents ovulation, thins uterine lining, lighter/more regular periods. | Often reduces pain, regulates cycles, can use continuously to skip periods. Widely available. | May not be strong enough for severe pain. Contains estrogen, which can be a problem for some. Side effects like mood changes, nausea. |
| Progestin-Only Therapies (Mirena IUD, progestin pill, implant, shot) | Thins uterine lining, can suppress ovulation. The IUD works locally in the uterus. | No estrogen. Mirena IUD can drastically reduce period pain/flow for 5+ years. The shot (Depo-Provera) can stop periods. | Side effects can include irregular bleeding, weight gain, mood swings. The shot can cause bone density loss with long-term use. |
| GnRH Agonists/Antagonists (Lupron, Orilissa, Myfembree) | Creates a temporary, reversible "medical menopause" by drastically lowering estrogen. | Can be very effective for severe pain unresponsive to other hormones. Gives the body a break. | Menopausal side effects (hot flashes, bone loss, vaginal dryness). Usually limited to 6-24 months due to side effects. Often needs "add-back" therapy. |
| Danazol (a synthetic androgen) | Suppresses ovulation and menstruation. | Can be effective for pain. | Androgenic side effects (acne, weight gain, voice changes, facial hair). Not commonly used first-line anymore. |
Hormonal therapies are a band-aid, not a cure. They manage symptoms while you're on them, but the disease can progress again once you stop. They also aren't an option if you're actively trying to conceive.
3. The Surgical Route: Laparoscopic Excision vs. Ablation
When medications fail or aren't an option, surgery becomes the talk. Not all surgeries are created equal. This is critical.
Laparoscopic Ablation (or Cauterization): The surgeon uses heat (laser or electricity) to burn the surface of the endometriosis lesions. It's like weeding by burning the tops off the plants. It can provide relief, but the roots often remain, leading to a higher chance of pain returning (recurrence). Many specialists now consider this an outdated approach for anything but the most superficial spots.
Laparoscopic Excision Surgery: The surgeon cuts out the endometriosis lesions completely, removing them root and all, like carefully digging out a weed. This is considered the gold standard surgical treatment, especially for deep infiltrating endometriosis. It requires significant skill and training. The goal is complete removal of all visible disease while preserving healthy tissue. Studies suggest it leads to better long-term pain relief and lower recurrence rates compared to ablation.
Finding a surgeon who is an expert in excision surgery is probably the single most important decision you can make if you go the surgical route. Ask about their specific training, how many excision surgeries they perform annually, and their philosophy on preserving fertility (if that's a concern). Don't be shy—this is your body.
4. Fertility and Endometriosis: A Complex Puzzle
If pregnancy is a goal, the treatment path shifts. Hormonal therapies that suppress ovulation are off the table. The focus turns to surgery to remove disease that might be blocking tubes or affecting ovarian reserve, followed by fertility treatments like intrauterine insemination (IUI) or in vitro fertilization (IVF).
Excision surgery can improve natural conception rates for those with mild to moderate disease. For those with severe disease or diminished ovarian reserve, IVF often becomes the recommended path. It's a complex, emotional journey that requires a coordinated team—a skilled endometriosis surgeon and a reproductive endocrinologist (fertility specialist) who understand the condition.
5. The Support Crew: Diet, Physical Therapy, and Mental Health
Medical treatments are one piece. Managing a chronic condition like endometriosis requires a whole-team approach.
Diet: There's no universal "endo diet," but many find reducing inflammatory foods (processed foods, red meat, sugar, gluten, dairy) can help ease symptoms. An anti-inflammatory diet focusing on fruits, vegetables, whole grains, and healthy fats is a sensible starting point. Keeping a food and symptom diary can help you spot your personal triggers (hello, endo belly!).
Pelvic Floor Physical Therapy (PFPT): This is a game-changer that's wildly underutilized. Chronic pelvic pain causes the muscles of the pelvic floor to become super tight and painful—a condition called hypertonic pelvic floor. A specialized pelvic floor PT can teach you techniques to relax these muscles through internal and external massage, stretching, and biofeedback. It can dramatically reduce pain with sex, urination, and general pelvic pain. If your doctor hasn't mentioned it, ask for a referral.
Mental Health: Chronic pain is exhausting and isolating. It can lead to anxiety, depression, and PTSD from medical trauma. Seeing a therapist, especially one familiar with chronic illness, or joining a support group (online or in-person) can be invaluable. Your pain is real, and your mental well-being matters just as much as your physical health.
Common Questions About Endometriosis (The Stuff You Actually Google)
Let's tackle some of the real, nitty-gritty questions people type into search bars at 2 AM when the pain is bad.
Does endometriosis go away after menopause?
Usually, yes. Since the disease thrives on estrogen, natural menopause (when estrogen levels drop) typically causes the lesions to become inactive and symptoms to improve significantly. However, if you're on hormone replacement therapy (HRT) that contains estrogen, it could potentially stimulate any remaining tissue. And for those who have had a hysterectomy but kept their ovaries, the disease can persist because the ovaries still produce estrogen.
Can you get pregnant if you have endometriosis?
Absolutely. Many women with endometriosis get pregnant naturally. However, it can be more challenging. The key is not to wait too long if you're struggling. If you're under 35 and have been trying for a year (or 6 months if you're over 35) without success, it's time to see a fertility specialist. Early evaluation and a tailored plan are crucial.
Is endometriosis an autoimmune disease?
It's not officially classified as one, but it shares many features with autoimmune disorders, like chronic inflammation and the immune system failing to clear the misplaced tissue. Research is ongoing in this area. Many people with endometriosis also have co-occurring autoimmune conditions (like Hashimoto's thyroiditis, lupus, or rheumatoid arthritis), suggesting a possible link.
What's the difference between endometriosis and adenomyosis?
They're cousin conditions, and you can have both (many do). Endometriosis is tissue outside the uterus. Adenomyosis is when similar tissue grows into the muscular wall of the uterus itself. It causes the uterus to become enlarged, boggy, and very painful, leading to extremely heavy periods and severe cramping. Diagnosis is often via MRI or ultrasound, and treatment options overlap but can differ (a hysterectomy is a definitive cure for adenomyosis, but not for endometriosis if ovaries remain).
Are there any new treatments on the horizon?
Research is finally picking up pace. Areas of interest include immunomodulators (drugs that target the immune system's role), angiogenesis inhibitors (drugs that stop new blood vessels from feeding the lesions), and more targeted hormonal drugs with fewer side effects. Non-hormonal pain medications specifically for endometriosis are also being investigated. Staying informed through reputable sources like the Endometriosis Foundation of America or the Office on Women's Health can help you learn about new developments.
Putting It All Together: Your Action Plan
If you're reading this and a lot of it sounds familiar, don't panic. Feeling overwhelmed is normal. Here's a practical, step-by-step way to move forward.
- Start Tracking: Download a period/symptom tracker app or use a notebook. Log your pain (scale 1-10), its location, bowel/bladder symptoms, fatigue, and when it happens in your cycle. This data is powerful ammunition for your doctor.
- Find the Right Doctor: Look for a gynecologist who lists endometriosis as a special interest or a fellowship-trained Minimally Invasive Gynecologic Surgeon (MIGS). Patient advocacy groups often have provider lists. Prepare for your appointment with your symptom log and a list of questions.
- Consider a Pelvic Floor PT Evaluation: Regardless of your surgical plans, this can be a huge help for pain management.
- Explore Your Treatment Options: Have an honest conversation with your doctor about your goals (pain relief, fertility, both) and start with the least invasive option that makes sense for you.
- Build Your Support System: Connect with others who get it. Online communities (like r/endometriosis on Reddit, but be mindful of misinformation) can make you feel less alone.
Living with endometriosis is a marathon, not a sprint. There will be good days and awful days. The goal isn't perfection; it's improvement. It's reclaiming as much of your life as possible from this condition. You are not just your pain, and your experience is valid. Keep advocating for yourself—you're the expert on your own body.



Leave a comment